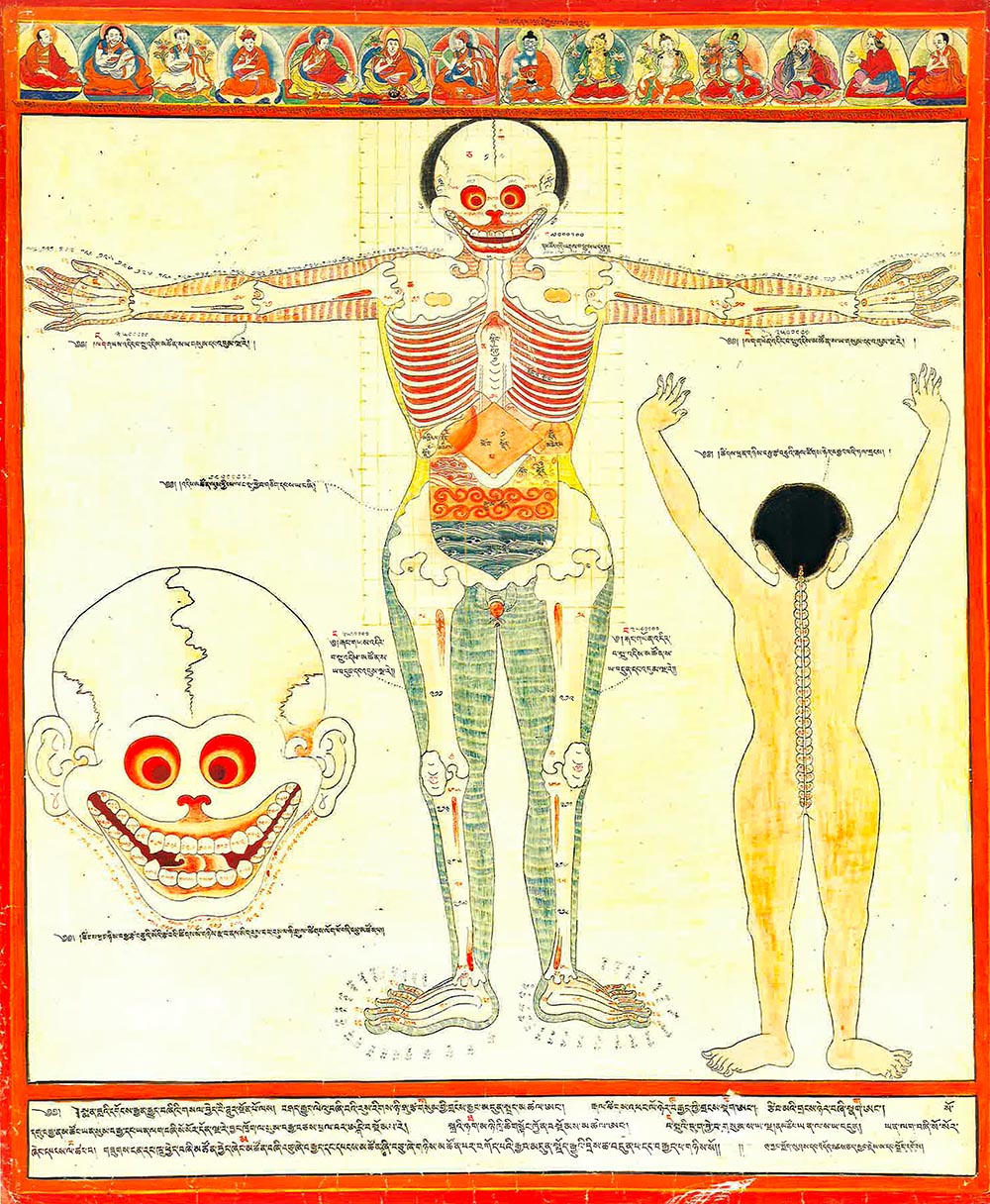
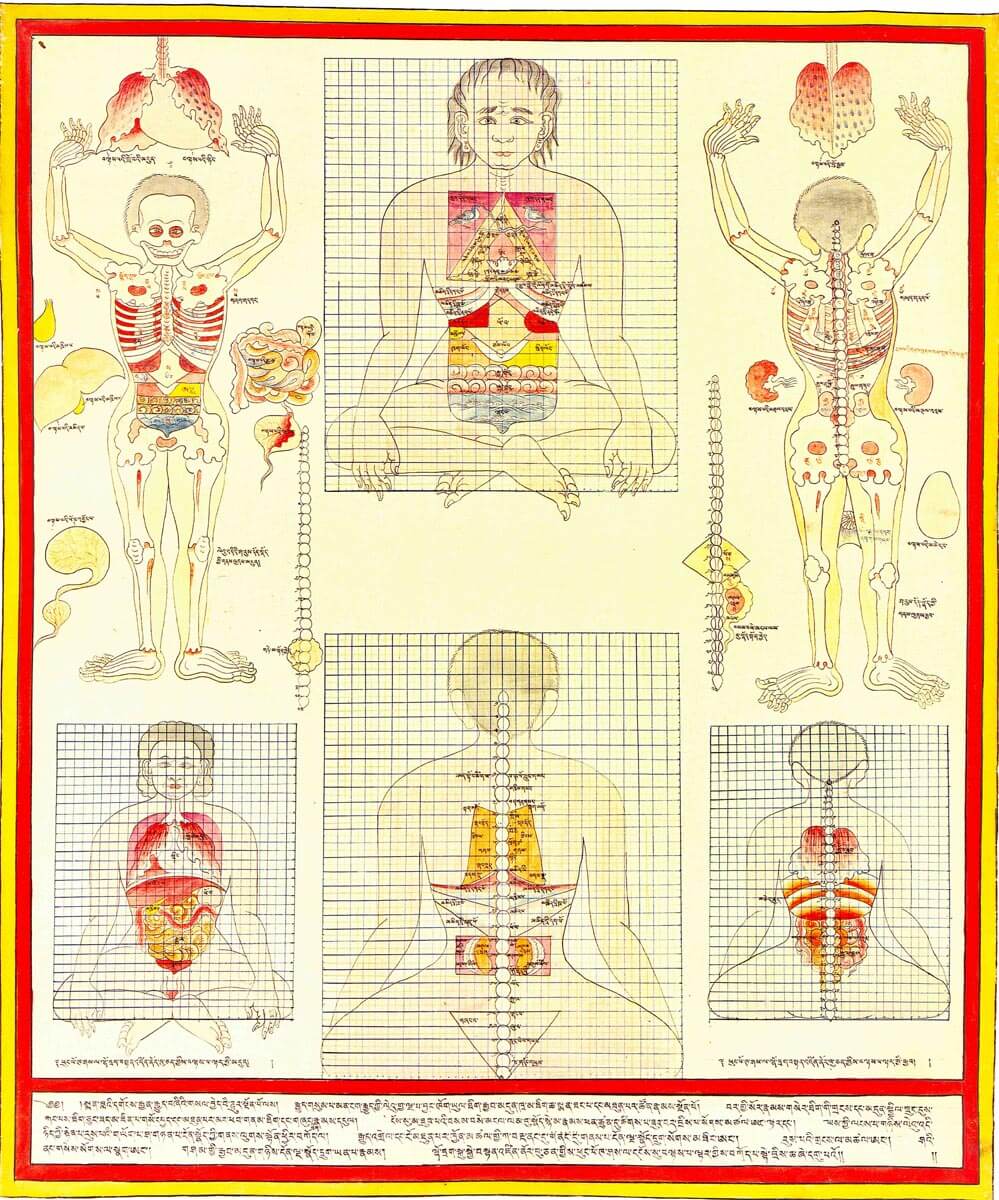
These Tibetan medical paintings can be understood as an extension of a broader iconographic painting tradition known as thangka originating in Indic Hindu and Buddhist cultures as a support for visualizing the ideal form in contemplative and yogic practice for soteriologically transformative aims. Similarly, these anatomical thangkas illustrate ideal medically functional forms vis-à-vis prescribed anatomical metrics
(Figs. 1, 2) and metaphor-based descriptions
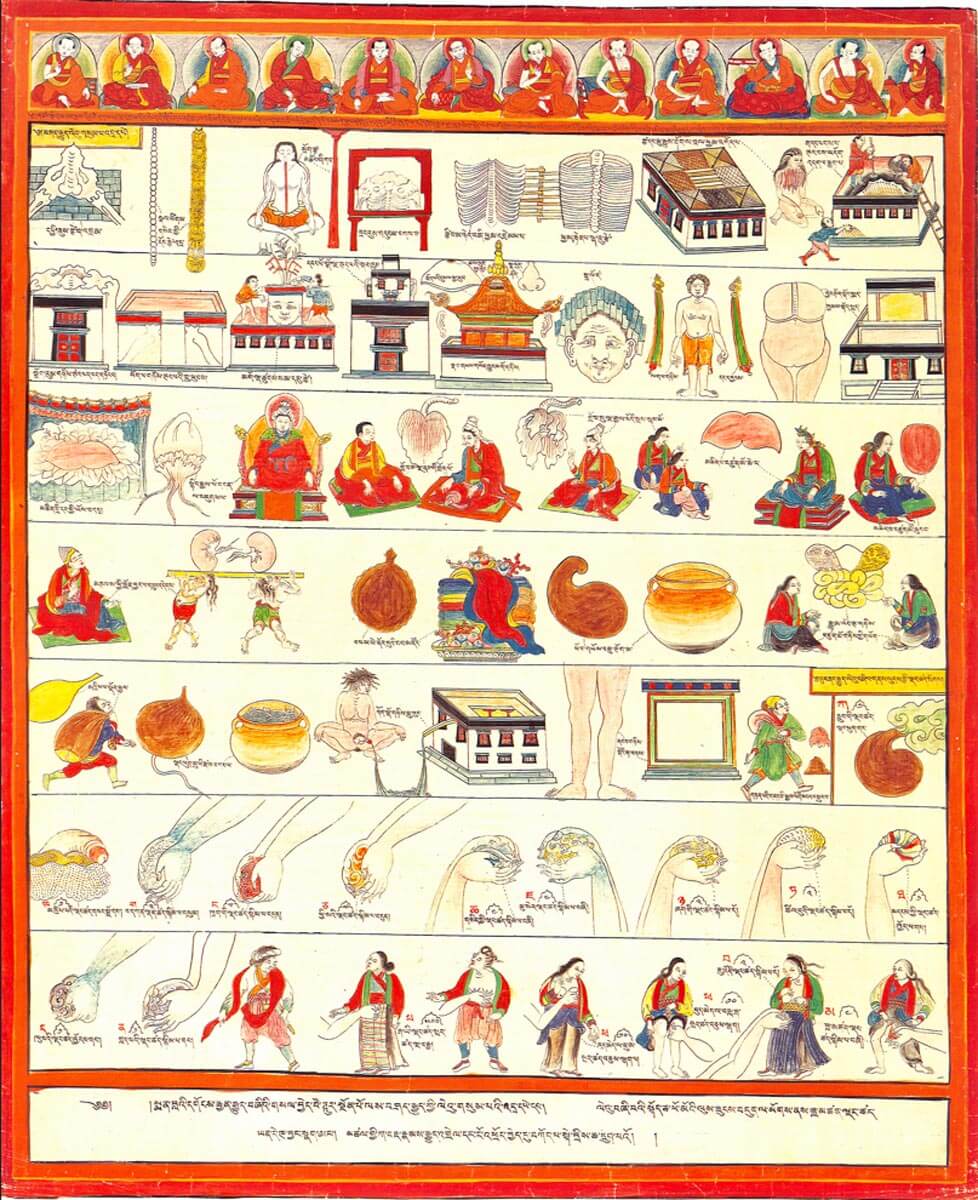
(Fig. 3). Quotidian details of facial expressions, householder and monastic contexts, and environmental and social ecologies
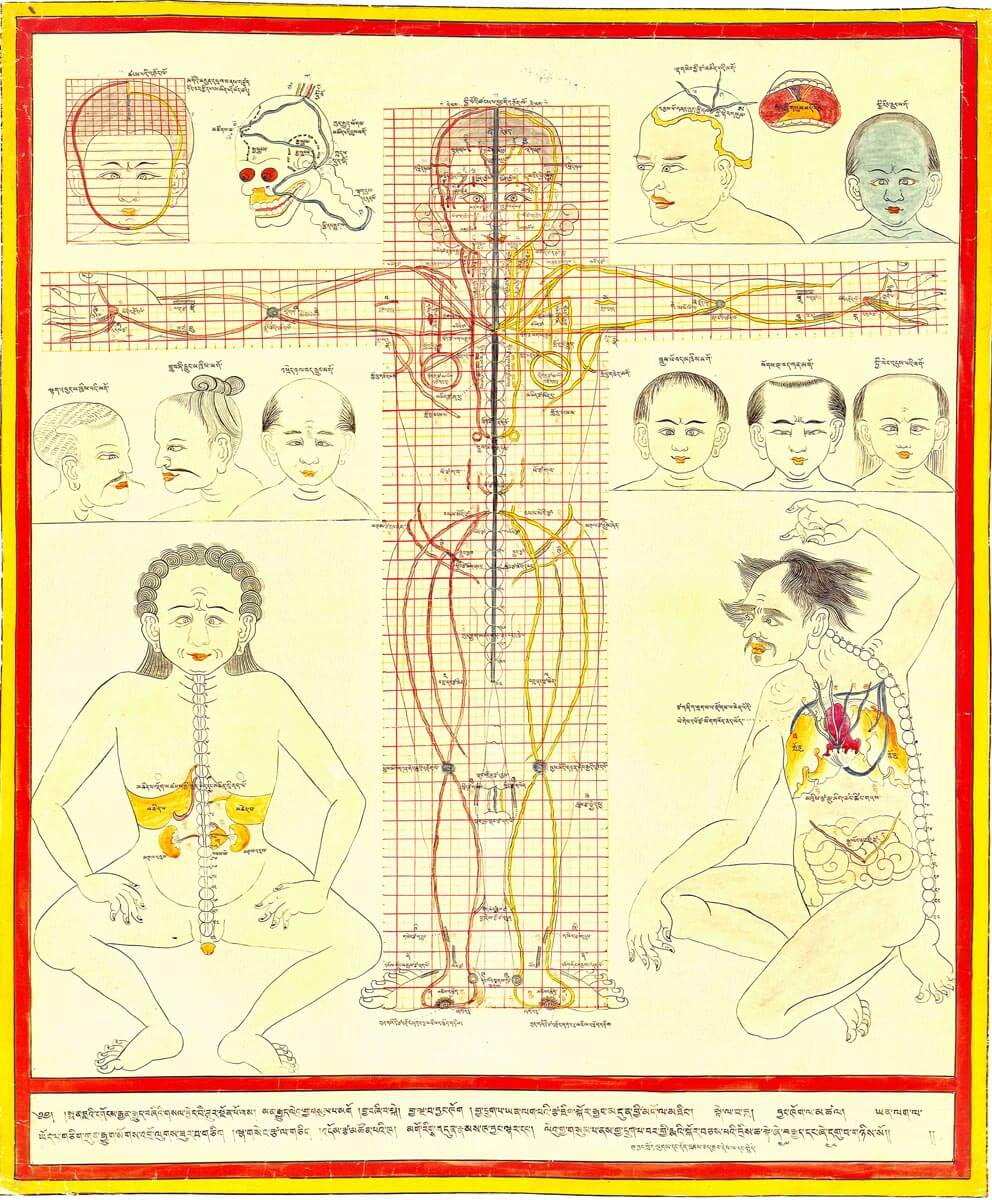
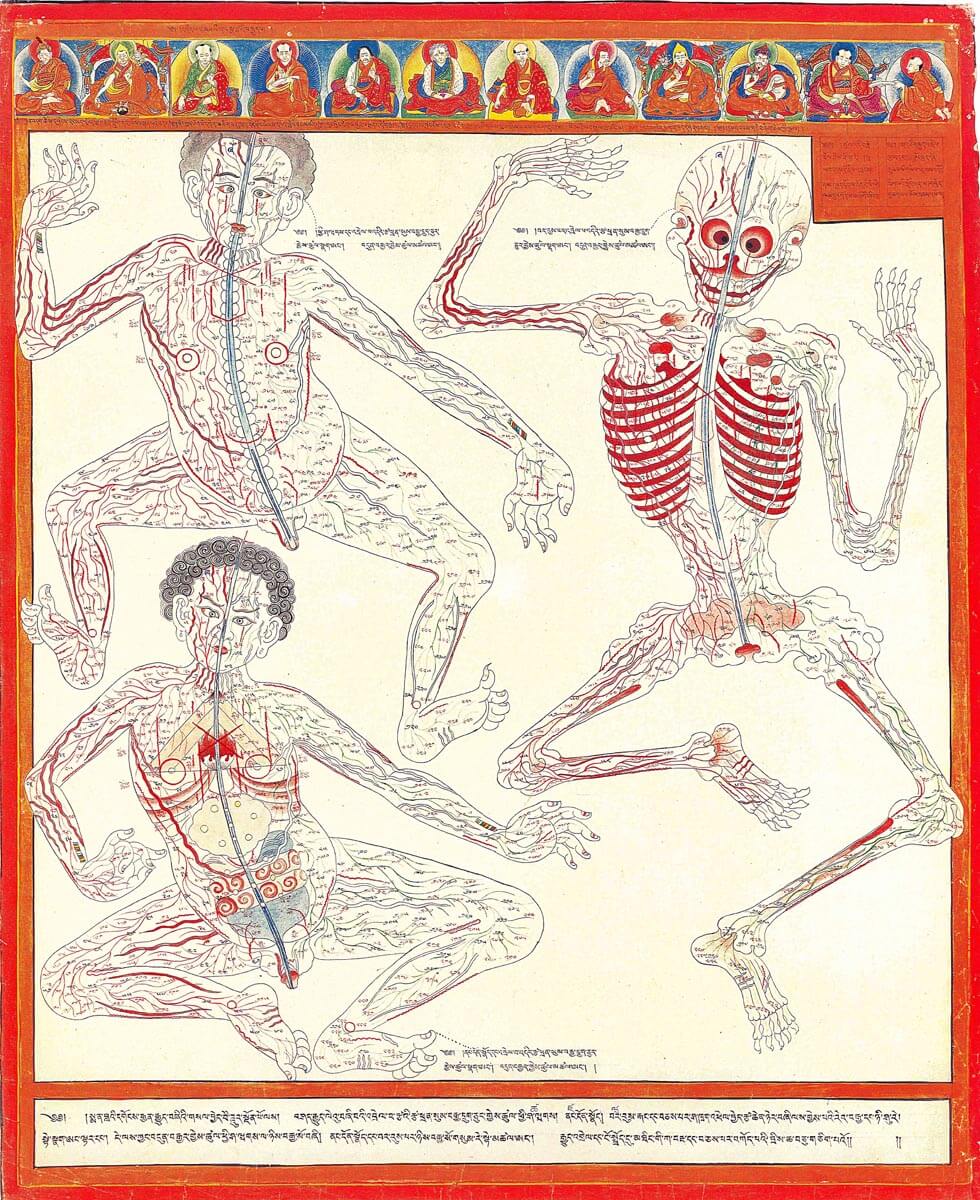
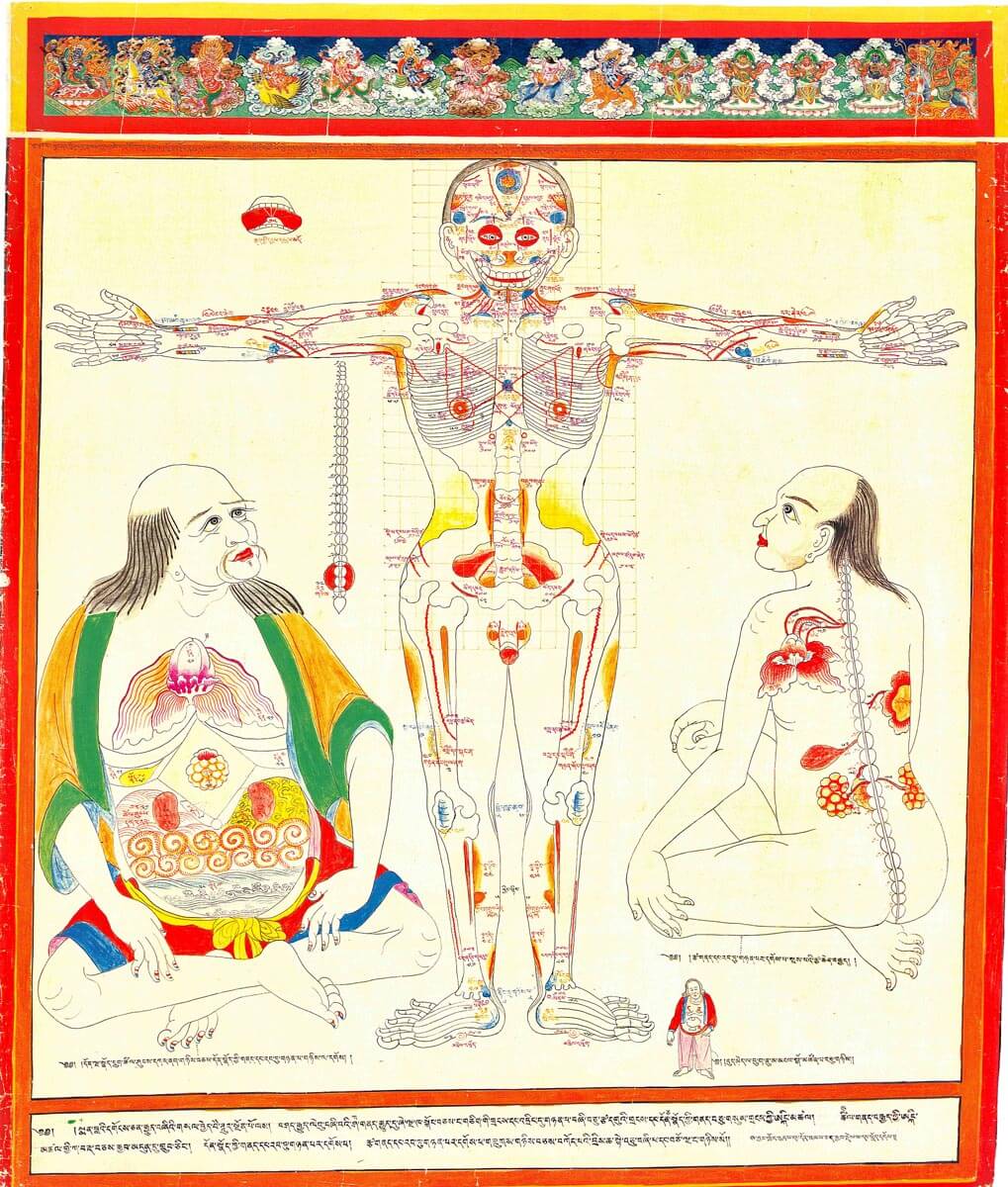
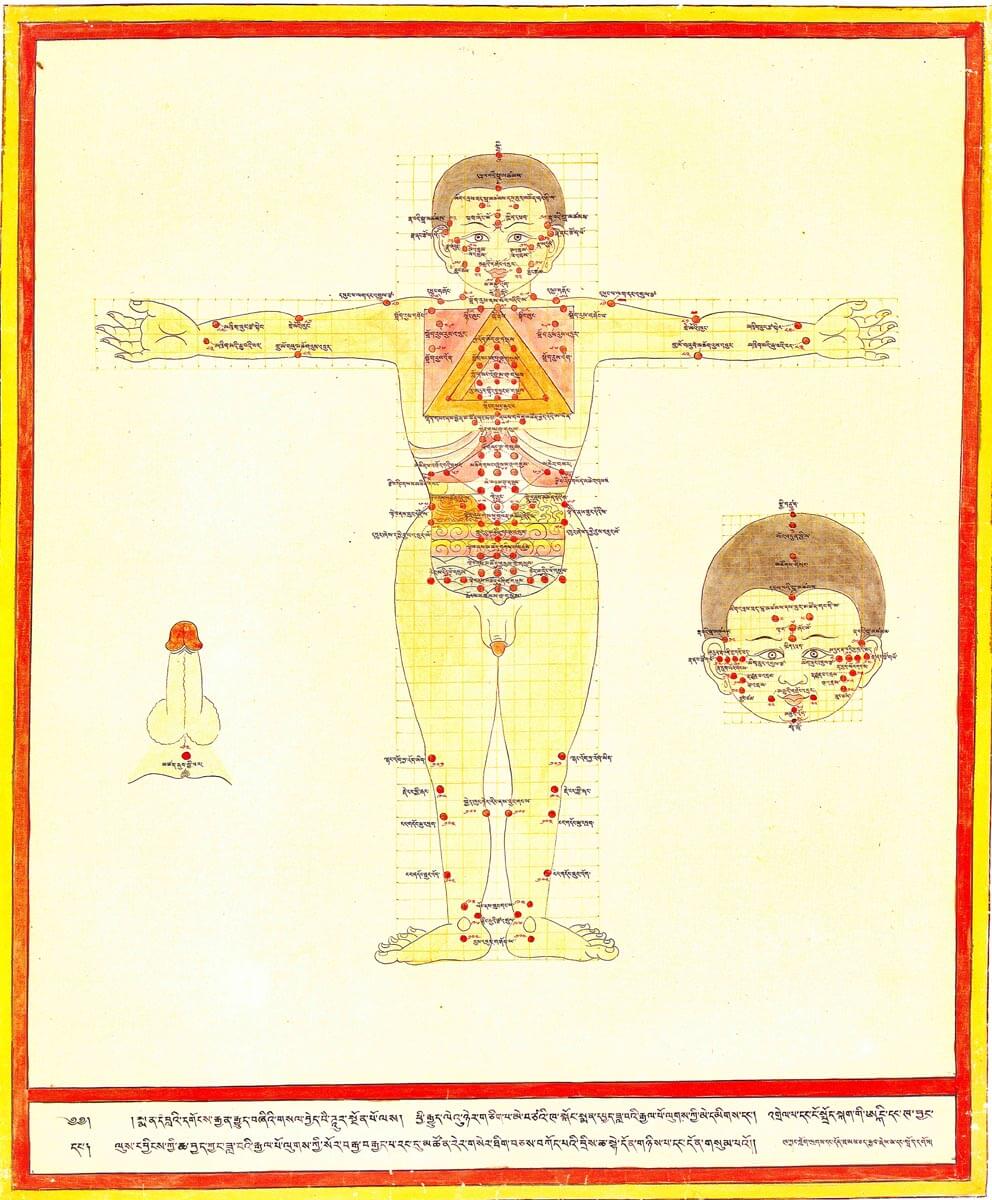
(Figs. 3, 4, 6, 8) represent naturalistic content physicians should understand to help patients cultivate health. The dual aims of the physician to support patient mundane wellbeing and salvific mind-body transformation are illustrated (e.g., coarse-subtle channel structures
(Figs. 4, 5); tri-color fingernails symbolizing three kāya bodies of Buddhahood
(Fig. 6)). Smaller medical drawings had been made in texts much earlier in Tibetan history to illustrate medicinal plants, critical treatment points, and anatomical details. However, Desi Sangyé Gyatso’s 17th century 79-painting commission formalized a new tradition of thangka. As visualized by the series, the most critically relevant structures for health and healing from the Tibetan medical perspective are the guts, channels, and their related interplay. The three gastrointestinal chambers and functional phases most critical to digestion—stomach, intestines, and colon—as well as the most relevant associations to liver and gallbladder are illustrated
(Figs. 1, 2, 4, 5, 6). Cupped hands
(Fig. 3) illustrate a measuring technique for proper amounts of fluids, including urine and faeces, normally produced by the body as described to be in proportion to an individual’s anatomy. Paintings detailing major and minor vasculature
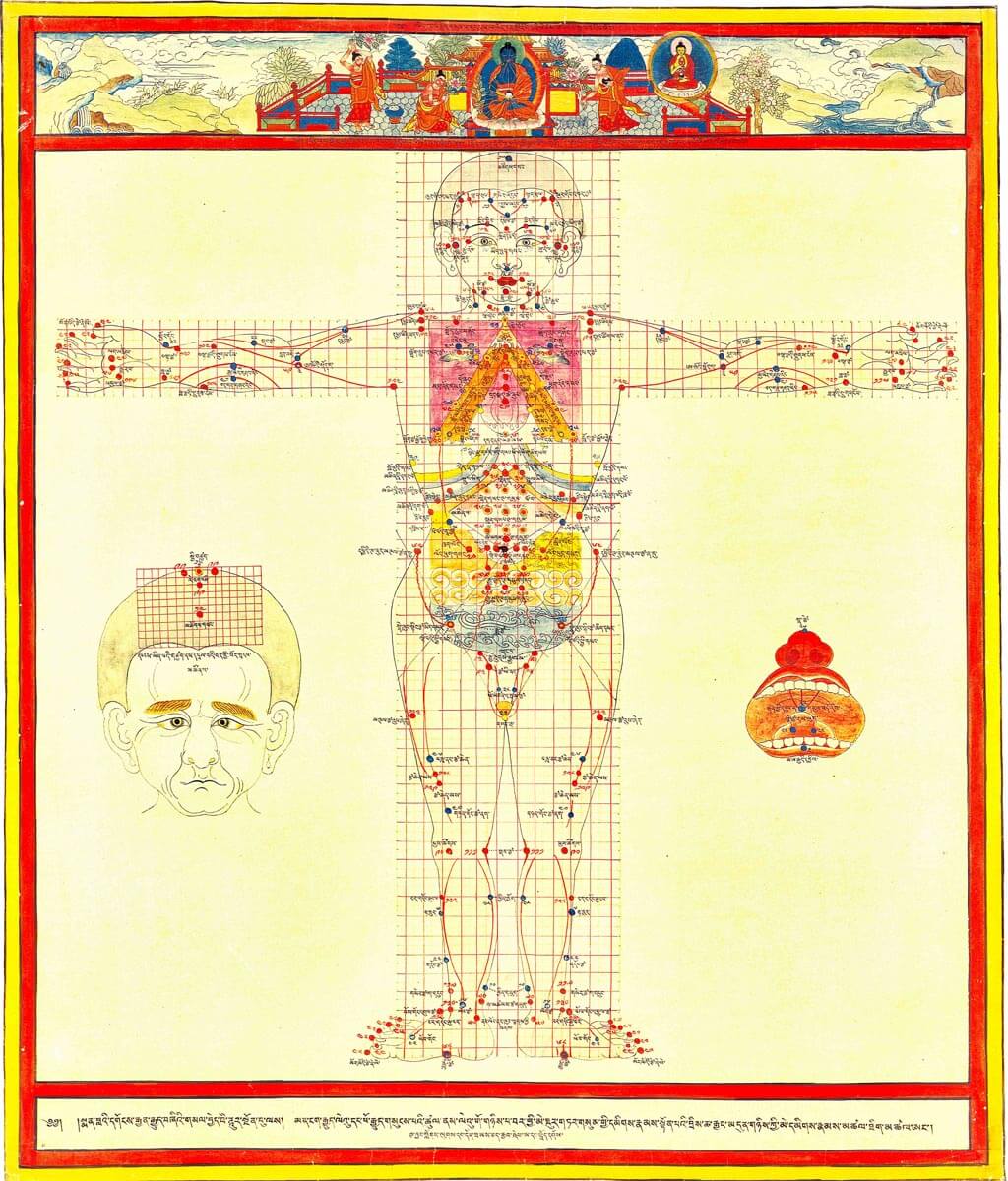
(Figs. 4, 5) and treatment points
(Fig. 7, 8) provide important visual supports to key paradigms for the gut, namely that all chronic disease results from impairment to the gut’s qualitative function of accessing nutrition and removing waste product. Disruption to normal metabolic processes, particularly when waste product enters the nutritional stream, known as
dangma mazhuwa, can develp into innumerable chronic conditions. Invariably such conditions involve poor synchronization of liver function and poor blood quality, at times therapeutically resolved through venesection of key points
(Fig. 7). Impaired gut function can also give rise to cancers and other neoplasms, edema disorders, ascites, arthritis types, and chronic inflammatory conditions like asthma, psoriasis, atopic dermatitis, and various gastrointestinal conditions. Moxabustion, or burning herbs on designated points
(Fig. 7, 8), is administered for a number of gut conditions, particularly those that are cold-natured. The gut interconnects with every part of the body through a rich channel network
(Fig. 4, 5)— blood, neural, lymphatic and interstitial. This vast integrated complex facilitates the body’s development, maintenance, and healing activities, as well as subtle associations with mind
(esp. Fig. 4). With the later spread of Buddhism towards the north, various medical schools were established in Mongolia and Buryatia, copies of the set were reproduced, and regional forms of visual interpretations emerged. In early twentieth century, shortly before the Stalinist purges began, a new school of artistic interpretation developed, particularly in Buryatia, based on integrating the Tibetan medical traditional approach with biomedical concepts. During the last two decades, a number of modern anatomical atlases have been published in Tibetan and Chinese-Tibetan. Contemporary renditions
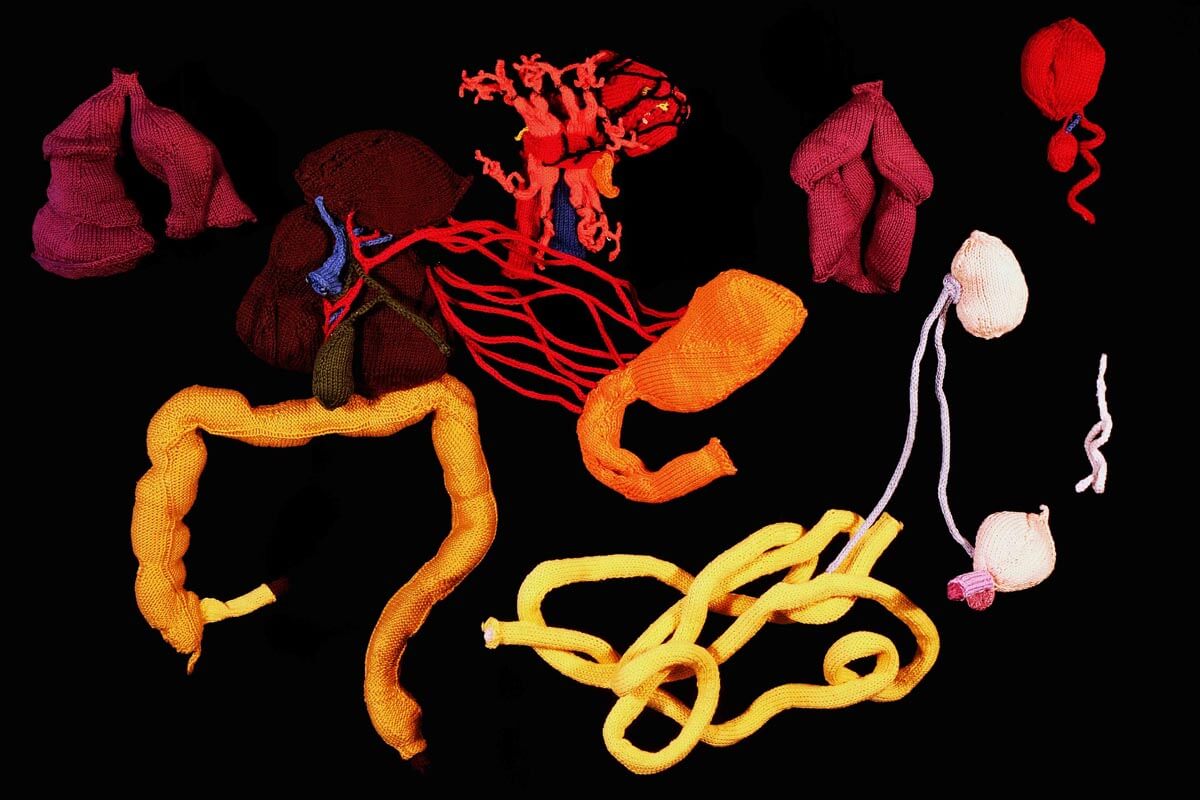
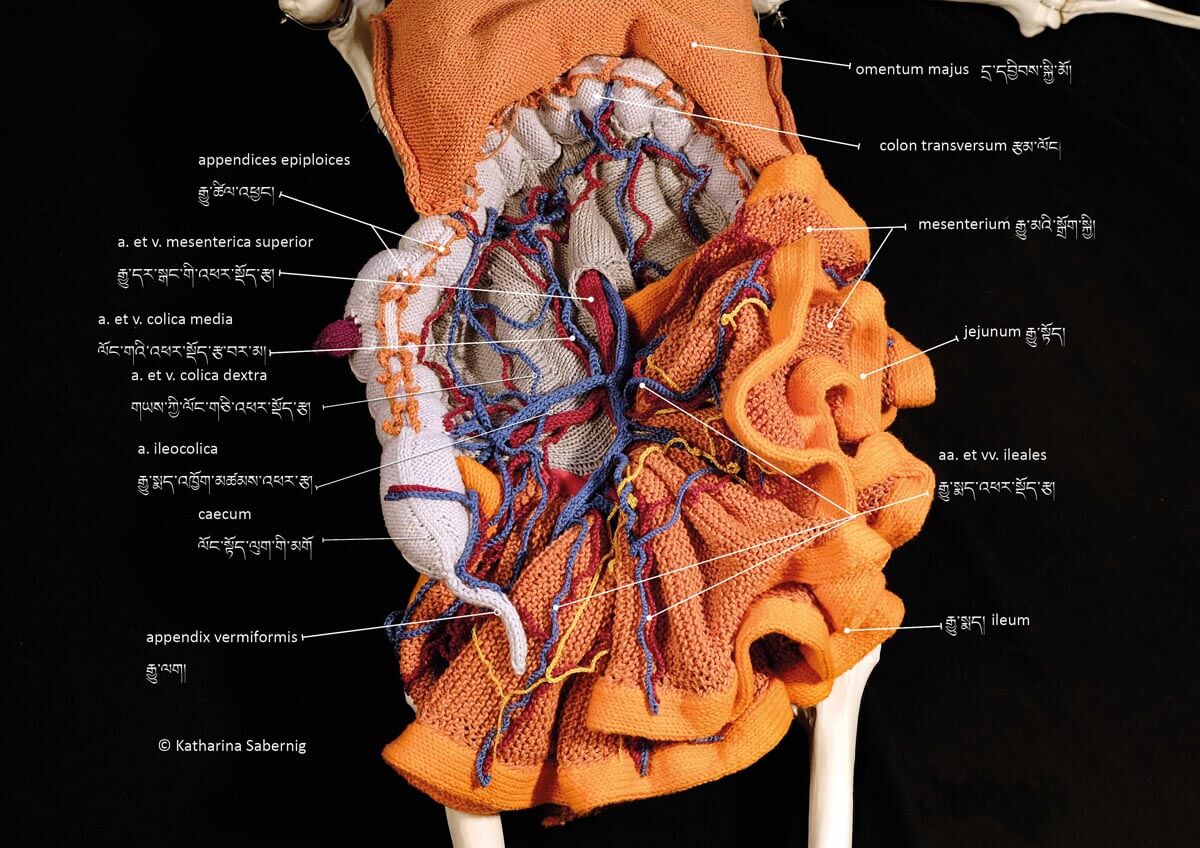
(Fig. 9, 10) represented by knitwork result from an interdisciplinary art project merging historical terms and neologisms with different modes of anatomical presentation by coauthor Katharina Sabernig.